It's Wednesday and we have discussion on a few topics today. The first relates to…
Academic freedom requires evidence and knowledge – not a desire for headlines
The University of New South Wales Business School seems to be making headlines for all the wrong reasons. They have (at least) two attention-seeking academics that are not helping the reputation of the University. The first, thought he was being smart by trying to put Modern Monetary Theory (MMT) down and lie about my own work only to make a fool of himself. I note that someone at The Conversation, which damaged its credibility publishing the piece, has now edited the original piece (taken my name out of the text). The stupidity of the attack on MMT remains however. I dealt with that in this blog post – When mainstream economists jump the shark and lose it completely (January 23, 2017). Now, another academic who thinks somehow she is a wonderful communicator bringing economics to the public, is causing a national debate about freedom of speech and all the rest of it. She is arguing that the Australia should not have followed its lockdown strategy, and, instead should have allowed around up to 25,000 Australians to die in order to protect the economy. So far, only 155 have died. The controversy is being constructed as one of free speech and academic freedom. But academics should only be free to make statements using their university attribution if they are based on evidence that can be supported. I don’t dispute the academic’s right to be provocative. I do dispute her command of the evidence and her ignorance of matters macroeconomic. That is the problem here. Short recommendation: I would not study economics in this Department.
As the reality of a pandemic was becoming clearer to me, I wrote this blog post – Learning about epidemics (March 25, 2020) – to help sort out my ideas.
I was seeing all sorts of Tweets from those claiming that the world’s increasing lockdown response was a dramatic overreaction to what was conjectured to be a nasty influenza episode.
I saw people holding out Sweden as a way forward and all sorts of arguments about herd immunity and all that sort of stuff.
It was early days in the pandemic. Iran had been devastated and I left Italy in February just a few days before their northern situation became a reality.
There were all sorts of statistics and ratios being quoted telling us that the death rate and the contagiousness was relatively low.
I examined various emerging databases that attempted to compare a bad flu season with what was going on with the coronavirus.
On February 26, 2020, we heard this from the US President – Remarks by President Trump, Vice President Pence, and Members of the Coronavirus Task Force in Press Conference:
The flu, in our country, kills from 25,000 people to 69,000 people a year. That was shocking to me.
They were reciting data from the US Centers for Disease Control and Prevention.
And if you were to make a comparison, the latest deaths from COVID in the US are 150,444 persons and the ‘season’ isn’t done yet.
But more thoughtful people understand that such a comparison requires like with like, which is not possible in this case.
This Scientific American article (April 28, 2020) – Comparing COVID-19 Deaths to Flu Deaths Is like Comparing Apples to Oranges – tells us that making such comparisons:
… are based on a flawed understanding of how flu deaths are counted, which may leave us with a distorted view of how coronavirus compares with it.
The evidence suggests that while the CDC was justified in:
… substantially overestimating flu deaths, in order to encourage vaccination and good hygiene, at this point the CDC’s reporting about flu deaths is dangerously misleading the public and even public officials about the comparison between these two viruses.
And that sort of erroneous analysis then leads to people claiming the lockdowns and the economic damage they are causing are unnecessary.
Careful analysis can provide some more accurate comparisons of the actual deaths from influenza relative to Covid.
The SA article concludes:
… we have to compare counted deaths to counted deaths, not counted deaths to wildly inflated statistical estimates. If we compare, for instance, the number of people who died in the United States from COVID-19 in the second full week of April to the number of people who died from influenza during the worst week of the past seven flu seasons (as reported to the CDC), we find that the novel coronavirus killed between 9.5 and 44 times more people than seasonal flu.
I was trying to do that sort of analysis myself in March 2020 and as far as I was able to get, given data limitations, my conclusion, outlined in the blog post cited above was that nations cannot allow this disease to run loose.
And that rather ‘naive’ conclusion, naive in the sense that we hardly knew anything about the virus – its contagiousness, longer term effects, how long immunity lasts, different impacts on different age cohorts (they were all calling it an old persons’ disease – they were wrong) – I think is supported by the evidence that has emerged since.
We still don’t know much about those questions – impacts etc.
What we know is that it is a very nasty virus that attacks all ages, is very contagious, and will decimate a population if allowed to run free.
Which brings me to Gigi Foster.
This ABC news report (July 28, 2020) – Heated Q+A discussion sees economist Gigi Foster deny she is ‘advocating for people to die’ – provides some information about this debate.
Foster has infuriated people by claiming that Australia cannot eliminate the virus from our nation and that the economic ‘costs’ are too large to try.
She appeared last night on the national broadcaster’s prime Q&A program and said:
If you look at what’s happening to those death counts around the world, in every country that has had a proper first wave, [they are] somewhere between 0.5 per cent and 0.1 per cent of the population …
That translates in Australia to about 12,000 to 25,000 deaths for people who are predominantly elderly or immunocompromised.
But it’s a body count.
You can see the segment on last night’s Q&A program – HERE
The official UNSW Twitter account distanced the University from her views.
I also note many people are advocating her being silenced by the University.
My views on that are clear.
Various politicians and others have tried to silence me over the years by putting pressure on my university to discipline me over public statements I make.
The rules are clear.
Freedom of speech for academics is a crucial part of an open society, a democracy.
One of the things I was taught when I was entering academic life was that I would enjoy ‘tenure’ (which in those days meant I could only be sacked for ‘gross malfeasance’, which included sexual predation and things like that) but I was only open to speak publicly in my university capacity on matters on which I had expertise and for which an evidence base could support my statements.
Thus there were two dimensions to me having ‘free speech’ using my university status to gain access to the public debate.
1. Expertise.
2. Evidence.
I differentiate this concept of ‘free speech’ to the broader rights that citizens have in open societies to say what they want within the constraints of discrimination and libel.
Value of Life concepts
Foster was just advertising why people should be careful in deciding to study economics.
Her comments were unsurprising to me given I have heard this sort of stuff all my career and particularly during my early years in postgraduate studies (microeconomics and welfare economics).
When I was a young academic, I was often commissioned by a major legal firm to provide expert testimony in worker’s compensation cases. This required me to estimate foregone earnings and other related parameters.
The opposing side always tried to reduce the size of the payout that the injured (or family of a dead) worker would receive.
They wheeled out the standard microeconomic analysis, which in this case, centred on the – Value of Life concepts.
The analysis comes up with a dollar value on a loss of a limb or life in total.
We would have to argue with sociopaths in the courts about whether lost legs, which destroyed the worker’s life quality and work opportunities, was worth x thousand dollars or y thousand, when the loss was infinite in terms of quality and decency.
It really was a daunting introduction to this sort of analysis.
And whenever I raise this issue, non-economists look at me in horror and say how can we tolerate that and all the other bleeding heart arguments (which should not be taken to conclude that I oppose them).
Then I tell them that the design of the road that they had driven on to work or leisure was based most likely on ‘Value of Life’ analysis. The road builders (state) cut their investments on the features of the roads that will reduce accident carnage and know there will be lost lives.
But to them the reductions in fiscal outlays (dollars) more than compensate for the estimated deaths per year or something that have been forecast from Value of Life studies of the road design.
Provision of health care is similarly blighted by this sort of analysis.
So I wasn’t surprised that Foster would implicitly have the same sort of reasoning.
In this sort of mentality, if the losses of GDP and related costs outweigh the estimated dollar losses arising from the deaths (persons times their ‘value’) then the lockdowns are unjustified.
That is the reasoning.
The presumption is that there is some inevitable trade-off between economic losses and deaths in this coronavirus crisis.
As this story from Wired (May 11, 2020) – How Much Is a Human Life Actually Worth? – notes:
… the choice seems stark: Continue strict social distancing and shelter-in-place measures to minimize the spread of Covid-19 and save thousands of lives, or end the lightweight lockdown-open all the shops, restart the factories-and save the economy.
I will come back to that later.
Some evidence
But Foster was pathetic on national TV last night when grilled about her views.
She claimed Sweden to be the example of the sagacity of her opinions.
She said:
I think that Australia can follow in the footsteps of many other countries in the world, some of which have not had lockdowns as strict as we have had here, such as again, Sweden – and look at the death tolls in those countries.
Yes, let’s compare the Australian and Swedish records over this crisis, which are summarised in the following table.
The Swedish – Covid Statistics – show that it has had 5,697 deaths from 78,997 confirmed cases. Its 2019 population was 10,348,730 in May 2020 (Source).
Australia’s – Covid Statistics shows 14,403 cases and 155 deaths. Australia’s population as at July 28, 2020 was 25,637,283 (Source).
| Country | COVID cases | Deaths | Cases per 100 thousand | Deaths per 100 thousand |
| Australia | 14,403 | 155 | 56.2 | 0.60 |
| Sweden | 78,897 | 5,697 | 763.3 | 55.05 |
Sources: Swedish Covid Statistics, .
Now the Arbetsförmedlingen (Swedish Public Employment Service) issued a report (July 13, 2020) – Arbetsförmedlingens verksamhetsstatistik juni 2020 – which provides the most recent unemployment data for Sweden.
We learn that:
1. 466,000 people were registered as unemployed, a rise of 130,000 over the last 12 months.
2. In terms of the official labour force, the unemployment rate had risen to 9 per cent (from 6.7 per cent a year ago).
3. The unemployment rate for females was 8.8 per cent and for males 9.2 per cent.
4. The unemployment rate for foreign-born workers in Sweden in June was 21.2 per cent and 5.5 per cent for domestic-born workers.
I analysed the latest Australian labour force data in this blog post – Australia labour market – one step forward up a gigantic mountain (July 16, 2020).
That data shows a very challenging situation for workers and I don’t want to understate that.
But compared to the deterioration in the Swedish labour market, it would be hard to say that the Australian labour market is in worse shape.
They are both in terrible shape.
So what is the return Gigi Foster thinks has accrued to Sweden as a result of its more ‘desirable’ approach to the pandemic?
It certainly isn’t coming in the labour market.
The real GDP forecasts for Sweden are also not flattering.
The latest forecasts from the Ministry of Finance, the central bank (Riksbank), various Swedis banks and the NIER are presented in this graphic (taken from this – IMF assessment).
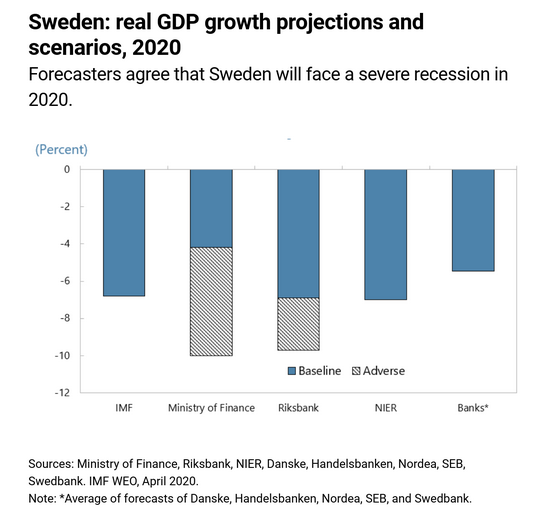
The latest forecasts for Australia – Economic and Fiscal Update July 2020 – show that:
Real GDP is forecast to fall by 33⁄4 per cent in calendar year 2020, the largest fall on official record, and fall by 21⁄2 per cent in 2020-21
That is a smaller projected fall than the range of forecasts for Sweden.
I wouldn’t quibble over a few percentage points – given the inaccuracy of these exercises – but there doesn’t seem to be any output payoff for Sweden.
Those seeking to defend Sweden’s track record deploy the ‘herd immunity’ argument and claim that Sweden will ‘recover’ more quickly as a result.
But even the IMF is cautioning against this sort of optimism:
Any final verdict will also depend on whether, as a by-product of its approach, Sweden is closer to achieving herd immunity, thereby increasing its resilience in the event of another wave of infection. Medical knowledge about Covid-19 is still accumulating, and recent tests indicate that immunity gains have been lower than initially projected.
This is the point about evidence.
Gigi Foster doesn’t know much about this disease. Even the medical experts are in the dark about many of the characteristics, especially the immunity issue and the long-lasting disabilities that ‘recovered’ patients may have to endure.
There is growing evidence that the impact on young people who acquire the disease is quite debilitating and may cause permanent brain damage.
And all the rest of the uncertainties.
I also thought it was interesting that even for economists who work within the standard framework, the lockdowns get the support.
Some US academics have published an article – The Benefits and Costs of Using Social Distancing to Flatten the Curve for COVID-19 (April 14, 2020) – in the Journal of Benefit-Cost Analysis, which examined the “net benefits of social distancing to slow the spread of COVID-19 in the United States”.
They found that:
1. “Social distancing saves lives but imposes large costs on society due to reduced economic activity”.
2. Without lockdowns, the GDP loss (present value) would be $US6.49 trillion, but the value of lives lost would be $US21.8 trillion (using the standard methodology).
3. With the lockdowns, the GDP loss would be $US13.7 trillion, value of lost lives $US9.41 trillion.
4. The net benefit in trillions of $US of the lockdown would be 5.16.
So even operating in the mainstream paradigm using its dodgy analytical techniques and methodologies, leads to a conclusion that the lockdowns made economic sense, notwithstanding the economic carnage that has been created.
Foster is correct in saying that there are life threatening consequences arising from the rising unemployment and lost incomes.
The ‘Value of Life’ concepts do not incorporate these difficult to measure ‘costs’. Clearly, the lockdowns have devastated peoples’ lives – their future prospects may have been severely compromised.
It is also too early to add up the health impacts of the coronavirus pandemic.
But here is where MMT comes to the fore
Most of this discussion would be passé if people understood Modern Monetary Theory (MMT) and realised that the sort of trade-offs that Foster is talking about are not inevitable.
And once you realise that, more ethical views on human life would come to the fore.
At the start of the crisis, I argued that the national governments, which issue their own currency, could take up the entire wage and profits bill if it wanted to – to reduce the ‘economic costs’ of the lockdowns to close to zero.
Unemployment did not have to rise.
Businesses did not have to be destroyed.
If we had an enforceable lockdown and eliminated the virus, with our borders strictly controlled until a credible health solution was introduced, then no economic damage was necessary.
Foster just adopts the neoliberal bias, that dominates the mainstream economics discipline, in assuming that if we have lockdowns there will be devastating GDP losses and elevated unemployment.
Once you understand the fiscal capacity of the Government then the concept of a trade-off seems rather flawed.
The economic losses that have been recorded to date – and they are massive – were avoidable.
They are not due to the lockdowns which were the sensible strategy for governments to adopt. I am thankful the Australian government took a relatively strict approach although I think they have relaxed the lockdown too early.
They did that because they were being confronted by the sort of nonsense that Foster peddles.
The economic losses arise because the governments adopted a flawed fiscal approach. They knew they had to expand fiscal deficits but were still thinking surpluses.
Our own Treasurer has even been channeling Margaret Thatcher in recent days – which means they are gearing up to further cut the already inadequate fiscal support.
If Gigi Foster understood macroeconomics she wouldn’t be making the sort of statements she has been making in the media.
Conclusion
I certainly believe that academics should be able to present their ideas to the public unfettered by university management as long as those ideas are within their expertise and are supported by research evidence that is held to scrutiny.
No university should seek to stop such speech on ‘commercial’ grounds (damage to their bottom line).
But in this current discussion, I do not believe that the evidential standard has been met.
Further, Foster’s intervention reveals her ignorance about macroeconomics
I also agree with New York Governor Cuomo who said:
To me, I say the cost of a human life, a human life is priceless. Period.
That is enough for today!
(c) Copyright 2020 William Mitchell. All Rights Reserved.
Seems to suggest what I suggested was likely to happen here some time ago – at the end of the day, the Swedish economy gets a whalloping ANYWAY – but with the added feature of large numbers of casualties that might otherwise have been avoidable.
“Short recommendation: I would study economics in this Department.”
Would or would not?
“(they were all calling it an old persons’ disease – they were wrong)”
The evidence from the Oxford CEBM and from elsewhere is that it kills old people disproportionately and more men than women. Under 40 and there is very little risk. Even under 50 there’s not a lot of impact. The median age of people dying is over 80.
The patterns are that it is a seasonal infection that follows the established patterns for seasonal respiratory diseases – possibly lagged by a few weeks. Which is why we’re heading into the danger period for Covid in Australia and NZ where outbreaks are probably going to become more likely as the season progresses.
Caution is advised!
But we have to be very careful to get it into proportion. We know lockdown is killing people too – the reported rise in stillbirths being one of the first indications (Up 5 per 1000, potentially up to 2000 infants lost so far here). A sensible graded Swedish approach with far better protection of people in elder care along with a heavy dose of MMT inspired fiscal activism would be my preference. (For example, let’s allow people over 60 to retire which allow them to keep out of harms way). I feel that balances freedom and risk the best and fits with the available evidence.
The current approaches give far too much succour to the rampant authoritarians in society of all colours. They are not going to want to give that power back once this fades away. I have a few East European acquaintances who are getting very jumpy about the current turn of events.
Protecting people while avoiding a descent into Authoritarianism is the challenge we face.
GDP be damned.
There still a general feeling in the supposedly progressive left that we in the UK should aim to be more like Sweden. However I would consider it to be mercantilist and we shouldn’t be advocating following their bad example. If they ever had found an attractive ‘third way’ they lost it again 20 or so years ago!
Mercantilism is embedded in the DNA of northern Europe, in particular Sweden, Germany, Holland and Denmark. Sweden has followed a diametrically opposite approach to Covid-19, compared to New Zealand and Australia. They have been attempting to run as normal, with mainly advisory messages around staying home and minimising physical socialisation. Sweden has been most explicit is arguing that the economy and their exports come first.
It’s easy to see how the others manipulate their currencies or use the euro to boost their exports but Sweden supposedly has a free floating Krona. But if it is free floating why doesn’t it rise to at least reduce their trade surplus? This was about 4% of GDP the last time I looked.
Just wondered if anyone had any thoughts on this?
I think Gigi’s comments are more about promoting Gigi.
Her comments will cost lives and will be used to undermine the public health effort.
Having an understanding of MMT in the general population to counter the neo-liberal nonsense is now a health issue, as social justice issue and an environmental issue.
Lately I wonder if these academic mercenaries are really ignorant or just spouting this mumbo jumbo only to evade the inevitable: that capitalism is nothing without the fiscal capacity of the state.
Like they fear we’ll wake up in communist totalitarianism if the government creates a few million jobs for a while. Or some other totally demented reasoning to keep unemployment up and wages down.
@Peter Martin
I hope you are not the Australian peter martin who co-hosts the show “the economists’ on abc RN with Gigi Foster. She certainly puts the lie to the idea that the world would be a better place if it was run by women…..
“But if it is free floating why doesn’t it rise to at least reduce their trade surplus? ”
The dynamic process of all Mercantalist currency areas is to capture Foreign currency assets on a balance sheet somewhere and then discount those into the local currency.
And that happens as the natural process of how FX works. You transfer your foreign deposit to the credit of the bank, and the bank simply marks up your local currency deposit at the current exchange rate. That process ripples up the banking chain as each bank discounts with the one above it in the money hierarchy, with the central bank doing precisely the same transaction for its member banks via “interventions”.
A quick glance of the Riksbank’s balance sheet shows it stuffed to the rafters with FX, all of which are “blocked deposits” as far as the FX currency area is concerned. That money is never going to be spent and provide somebody with an income in the net import areas.
The result is that the SEK exchange rate remains low and Swedish exports are maintained – draining demand from whoever they are exporting to.
“A sensible graded Swedish approach with far better protection of people in elder care *along with a heavy dose of MMT inspired fiscal activism* (my emphasis) would be my preference” (Neil Wilson).
That caveat (emphasised) seems to me to stultify your preferred prescription. Absent the wished-for “heavy dose of MMT inspired fiscal activism” what would your preference be? Seeing that so far as I’m aware nowhere in the real world, either in Sweden or anywhere else, is it currently in evidence.
Presumably not the same as the one you identify given its presence?
Have I understood this correctly? Is this official MMT doctrine?
Prof Mitchell seems to be claiming that that lockdowns have infinite benefits and zero costs.
“I say the cost of a human life, a human life is priceless. Period.”
In other words, the benefits of lockdowns are infinite if just one death is avoided.
.
“no economic damage was necessary”
“The economic losses that have been recorded to date – and they are massive – were avoidable.
They are not due to the lockdowns”.
“Mercantilism is embedded in the DNA of northern Europe, in particular Sweden, Germany, Holland and Denmark”.
Yes, and Finland (and a few others, eg Luxembourg?) too.
And how about Switzerland?
It seems to be correlated (though I’ve no idea to what if any degree of significance) with Lutheranism or, more broadly, Protestantism.
“The current approaches give far too much succour to the rampant authoritarians in society of all colours. They are not going to want to give that power back once this fades away” (Neil Wilson).
I seem to remember that there were plentiful signs of that during the war.
Those faded away pretty quickly after it ended though.
Admittedly, British society has radically changed (for the worse, naturally!) in almost every conceivable way since then so your forebodings may be warranted for all I know.
Bill : “(January 23, 2107).” in the opening paragraph?
What will make a good line of attack on MMT?
Now let me think like a right-winger at which I’m not particularly good.
I know you must be a commie wanting government to takeover all the economy. That was the line of attack against the Roosevelt Keynesianism which continued after the war. McCarthy made that a very vicious form of attack on government having any money of its own.
Now you get a watered down version from the likes of Simon Wren-Lewis and Thomas Palley that MMT can’t be technically correct because it has no maths in it. Noticeably they produce no logical mathematics to prove government has no money of its own to prove their point just like Margaret Thatcher produced no monetary system explanation for the UK to prove that it didn’t relying on people’s primitive resentment of tax to trigger support for her statement!
Why do I feel I live in a world of semi-educated apes who fail to recognise democracy is interdependent with a monetary economy?
Bill hits the bottom line of this new pandemic with this observation, which should be obvious to all who have attempted to keep up with the emerging, shifting data: “Even the medical experts are in the dark about many of the characteristics, especially the immunity issue and the long-lasting disabilities that ‘recovered’ patients may have to endure.” The conclusion necessarily follows that our societies should continue to err on the side of caution if they are to fully protect public health. Bill also hits the bottom line about the financial devastation that such caution-based policies will bring to many under neoliberal conditions: “At the start of the crisis, I argued that the national governments, which issue their own currency, could take up the entire wage and profits bill if it wanted to – to reduce the ‘economic costs’ of the lockdowns to close to zero. Unemployment did not have to rise. Businesses did not have to be destroyed.” I doubt whether there’s really much more to say about this mess we’re in, except to keep repeating these points until they finally sink in; i.e., that in addressing the Covid Crisis, MMT had already provided, in the economic arena, “the vaccine or effective treatment” we await in the health arena. There was no reason whatsoever, and there remains no reason, to pile an economic crisis on top of a health crisis. Much about the plague of Covid we have yet to understand, but we know all we need to know about the plague of neoliberalism.
Some of the questionable criticisms about the way this disease is being managed, put forth by various academics and others will soon be tested in a court of law.
A lawsuit has been launched in the Superior court of Ontario, Canada against the Federal government, the Government of Ontario, the Mayor of the City of Toronto, and the publicly owned Canadian Broadcasting Company.
A number of allegations are made in a fairly lengthy statement of claim which was recently read to the court by Canadian constitutional lawyer Rocco Galati, according to statements he made in a recent interview accessible via youtube.
It will be interesting to follow since it promises to present precisely formulated questions with supporting evidence regarding the non-constitutionality of some emergency measures, suspension of some rules of democratic procedure, the presentation of false/ misleading information to the public by the media, the censorship of relevant professional voices who publicly question the data collection methods, and the harm caused by the response to the virus (both medical and economic) vs the harm the virus itself causes.
Canada has experienced relatively few cases of the virus to date, and the government data we have seen so far, seems to suggest that as the lock down rules loosen, the cumulative case count rises, and visa versa.
The virus spreads very rapidly were population densities are greatest and proportionately less in less populous regions.
There is no doubt the elderly who are housed in long term care facilities, mostly privately owned these days, are the most at risk, of infection with life threatening illness. This has been in part attributed to part time or under payed staff working in more than one facility to make ends meet, and the lack of isolation due to room sharing.
There were cases of staff quitting work due the high risk of contracting the virus inside the facility. The military were brought in to provide support in some of those facilities with the consequence of numerous soldiers contracting the virus as well.
There have needless to say, been many calls for placing long term care within the the public health system since many of the salient issues seem to revolve around the financial concerns of private operators focused on profits. It is not guaranteed, that a public system under neoliberal guided, fiscally constrained, provincial management would offer any improvements over the long run.
Least, but still impacted are school age children, were there seems to be growing support from pediatricians who have been studying the evidence, for returning to school, and removing social distancing/masking requirements on the basis of harm reduction.
The longer this goes on, the clearer it should become about what actions are best, but the ability to make decisions and act on incomplete/ imperfect information is a necessary attribute to any form of leadership.
Typical heartless academic.
Wuhan eliminated the virus in 3 months! China can’t even test their vaccines because there are no infections. We exceed total infection cases in Wuhan every two days in the USA!
Just ignore the real world. No problem.
Stop whining and start realizing your neoliberal government, academia, and businesses have all failed your countrymen and women.
@Neil Wilson
Some months ago, you and I differed here on this blog as to how we should approach this issue (apologies if I have mistaken you for someone else).
While I have no formal training in either economics or medicine, as we can see the situation has nonetheless generally evolved in much the way I expected. The Swedish approach has resulted in a significantly higher cost in human lives for no particular tangible economic benefit. It should therefore be rejected as a viable approach.
“The evidence from the Oxford CEBM and from elsewhere is that it kills old people disproportionately and more men than women. Under 40 and there is very little risk. Even under 50 there’s not a lot of impact. The median age of people dying is over 80.”
I observe that the above statement is technically correct but focuses on individual outcomes while ignoring the COLLECTIVE outcome – which is a serious oversight and may lead to a significant underestimate of the end consequences.
Because how likely a disease is to kill an “average” individual is only part of the story of how many people it may end up killing. The other major factor is – how INFECTIOUS is it? How many people are likely to end up contracting it?
Rabies is an extremely lethal viral infection – untreated it is usually fatal. An individual person infected with Rabies is vastly more likely to die than an individual who contracts Covid-19. Yet the annual global death toll for Rabies is around 50 000 while Covid-19 has officially killed well over 10 times that number in about 6 months.
The reason that the milder disease is killing so many more people than the deadly one is obvious yet is regularly overlooked – as far as infectiousness goes, Rabies is pretty hard to catch. You need to be bitten or scratched by an infected animal. It can also be successfully treated if caught in time. So Rabies has no ability whatsoever to sweep through the population and infect millions (barring some Alfred Hitchcock-type scenario).
Covid-19 sits at the opposite end of the infectiousness spectrum to Rabies – this is an extremely contagious bug. You don’t need to be bitten or engage in unprotected sex in order to contract it, you merely need to be in close proximity to an infected individual who is coughing, sneezing or even speaking. And you may then in turn pass it on just as easily. This bug is capable of doing something that many more lethal diseases are not – running through the population like a fire out of control. And at this point in time, there is neither a vaccine nor a cure.
Each individual infection is a spin of the roulette wheel – the odds of it landing on a particular number may be low…….but spin the wheel millions of times and see what result the law of averages ends up delivering. This is what makes Covid-19 sufficiently dangerous to justify some fairly extreme containment measures. To say nothing of the emerging evidence of not-insignificant numbers of people being left with long-term health effects, some of them serious.
However, I understand the motivation underlying your position now – though I think there is little likelyhood of this occurring in places like the US or Australia.
@ Neil Halliday,
No that’s not me!
@ Neil Wilson,
Thanks for the comment. I’d guessed they must be doing something! So, that this kind of interventionism in the FX markets must mean that the Krona isn’t really a floating currency at all.
@Neil Wilson
“We know lockdown is killing people too – the reported rise in stillbirths being one of the first indications (Up 5 per 1000, potentially up to 2000 infants lost so far here).”
Interesting as we in NZ are finding:
“The number of babies born prematurely plummeted during the coronavirus lockdown….dropping by almost half”
Stuff NZ
“Coronavirus: Drop in number of premature births over lockdown”
The drop in premature births is also a feature – alongside the rise in still births. The two co-exist.
Just as well I noted it then Neil as you forgot to mention it.
“The Swedish approach has resulted in a significantly higher cost in human lives for no particular tangible economic benefit. ”
Except that it hasn’t has it. Swedish deaths per million are lower than Belgium and the UK – both of whom had lockdowns. And of course Peru, which had the hardest lockdown of all.
The variability across the world isn’t related to lockdown. It is related to other factors most of which we probalby haven’t discovered yet.
“Covid-19 sits at the opposite end of the infectiousness spectrum to Rabies – this is an extremely contagious bug.”
And yet the figures don’t bear that out. Because although it is very infectious, it is only very infectious to those who are susceptible. The underlying assumption in a great deal of models is that 100% of the population is susceptible. The data paths we have suggest that isn’t the case. Hence why *all* the projections about Sweden have been incorrect. Since they were incorrect, we can discard the assumptions in those models. That’s how science is supposed to work.
The models that fit the data we have better have more realistic mechanisms for dealing with both susceptibility and connectivity. Or as the academics put it
(Aguas, R. and co-authors: Herd immunity thresholds estimated from unfolding epidemics” medRxiv 24 July 2020 10.1101/2020.07.23.20160762)
“Just as well I noted it then Neil as you forgot to mention it.”
And? Do you have comparative statistics? Stillbirths are definitely dead who may have had a chance at life. Are you trying to counter that for some reason?
You haven’t mentioned Accident Latrogenics, Cardio Diabetes, Alzheimers, Stroke Access, Flu and Pneumonia, Cancer Access, or Suicide Addiction abandonment and abuse. How far would you like to go?
@ Neil Wilson,
Many thanks for giving the reference to an amazing new paper on Herd Immunity.
The paper is not yet peer reviewed but to my superficial eyes it appears to be mathematically brilliant and extremely important for policy. The paper concludes:
“In all four countries considered here [ Belgium, England, Portugal and Spain] we foresee HIT [Herd Immunity Threshold] being achieved between July and October and the COVID-19 epidemic being mostly resolved by the end of 2020.”
No more need for lockdowns and social distancing!
Hallelluya!
@Neil Wilson,
Not only is Covid-19 *NOT* seasonal like the flu, but evidence is emerging that the long term effects from even mild infection are considerable, and include heart, lung, and brain damage, which may well be permanent and lead to disability and lower life expectancy in patients, many of whom are in their forties.
A rapid death following acute infection may only be a small fraction of the attrition caused by Covid-19.
NB. Sadly this good news does not apply to countries like China, Australia, New Zealand, Taiwan, Hong Kong, Philippines, Iceland etc. which are largely successful in suppressing the virus. These won’t develop herd immunity until an much later date (or a vaccine).
When I first watched Gigi Foster’s analysis of the pandemic back in April, I cringed. However, I have to acknowledge that many of her predications about the harmful social consequences of the pandemic are proving to be right. The stress from the pandemic is relentless, cumulative and crippling.
The questions the pandemic pose are much deeper than simply whether to lockdown or not.
The national psyche of every country in the world is undergoing its own psychoanalysis, where social, cultural, and economic values are being examined and challenged.
While we might theorise over better ways to manage the crisis, the reality of the daily tectonic ructions remains an inescapable fact. There is something about the agony and tragedy that seems almost inevitable.
MMT enlightenment, on its own, was probably never going to bring down neoliberalism. Radical change was going to need a radical catalyst, one like COVID-19.
The implications of the pandemic extend far beyond economics.
Each of us can do no more than play our part as we see fit. (And Gigi really should acquaint herself with MMT.)
I heard Gigi on RN in the early days of the pandemic make her case for staying open. She argued we should be considering the downstream costs, but gave no data to support her argument. She was also arguing, as many did early on, for herd immunity.
I was very surprised to find that she hasn’t changed tune at all since then, despite 1) the virus proving to be worse than we had imagined, 2) the clear evidence that the Sweden approach failed, and 3) no country is even close to herd immunity.
Tomas Pueyo did a thorough analysis of herd immunity and the Sweden example back in June, well worth reading.
https://medium.com/@tomaspueyo/coronavirus-should-we-aim-for-herd-immunity-like-sweden-b1de3348e88b
The whole response to Covid19 has been a shambles, we seem to have forgotten what we did in the past. The lockdown was required to keep the hospitals from being overloaded but it shouldn’t have come to that, our response was to an influenza outbreak where antivirals could be used, we didn’t have a plan for a SARS type pandemic.
We used hospitals to treat a very infectious disease which made hospitals & care homes the centre of the outbreaks (think MRSA etc that you can only really get in a hospital). I think but not sure as I am going by anecdotes that people were (rightly) scared away from them and other procedures being put off (Lost my Mother In Law in June to cancer as she hadn’t been diagnosed). They built the temporary Nightingale hospitals but then practically didn’t use them.
Every day I cycle across what was the Joyce Green Hospital grounds just outside London, this was the isolation hospital for London particularly for smallpox. In those days they didn’t do the insane thing of putting infectious patients inside general hospitals. Our ancestors only a couple of generations back knew what to do, we have lost that.
@Kingsley Lewis,
The concept of “herd immunity” relies on any immunity to SARS-COV-2 conferred following infection being long-term or permanent. There is, as yet, no evidence that this is the case.
Immunity to SARS-COV-2 may well be only be short term, and/or to just one variant – of which there are now many.
The question has also been raised as to whether the massive auto-immune response (“cytokine storm”) seen in some of the sickest patients is a form of ‘allergic reaction’ to a previously encountered virus. If that were the case, then future exposure in supposedly “immune” patients to other variants of SARS-COV-2 may also induce this extreme, and often fatal, auto-immune response.
The most cautious and wise approach (such as seen in NZ) would therefore appear to be national elimination, followed by global eradication – as is the policy towards polio.
We don’t try to “live with” polio – why should we accept “living with” Covid-19?
The recent changes to death certification protocols in various countries have had a significant impact on reported COVID-19 mortality rates within those regimes. Environmental and containment factors alone will not explain the wide variation in morbidity outcomes.
@ Neil Wilson
“‘The Swedish approach has resulted in a significantly higher cost in human lives for no particular tangible economic benefit.’ (Leftwinghillbillyprospector)
“Except that it hasn’t has it. Swedish deaths per million are lower than Belgium and the UK – both of whom had lockdowns. And of course Peru, which had the hardest lockdown of all”.
Not to argue the point but for the avoidance of doubt:-
Swedish (and the other cited countries’) deaths, per million *what*, exactly?
Per million cases? Per million head of the population?
The difference is not trivial, I believe.
Cases are a function of testing. Testing outcomes are highly controversial. Therefore the relationship between testing and cases is controversial. The ratio of deaths per million population is more solid. The caveat of specifically introduced changes to death certification in some regimes is also significant in any morbidity ratio.
“Per million head of the population?”
^ From worldometer. Regrettably bodies are the only hard data we have. Deeply disturbing.
“Not only is Covid-19 *NOT* seasonal like the flu,”
It’s very seasonal. The patterns follow seasonal respiratory peaks and troughs for the latitudes of the areas – possibly with a lag. One of the reasons why tropical areas have suddenly spiked. The data paths are uncanny matches for the graphs in seasonal respiratory literature. The daddy being “The Transmission of Epidemic Influenza – R Edgar Hope-Simpson”
There are indeed people who have suffered terribly from this disease and will have ongoing health issues due to it. But similar effects come from Influenza and other respiratory diseases, as it says in the reports “The NHS said that figure might be accurate if COVID-19 follows patterns of similar diseases.”
The levels of those impacts and how many will be affected are unknown at this time which is why there are several long term follow up studies to assess the recovery of patients – particularly those who have been in intensive care.
Get to the primary source and read past the “please can I have some more money to study this” propaganda hook.
What is the hard evidence that any sort of immunity is possible with C19 let alone herd immunity?
“SARS-CoV-2 infection induces robust, neutralizing antibody responses that are stable for at least three months ” Wajnberg et al. 10.1101/2020.07.14.20151126
So will 3 months personal immunity support herd immunity or is permanent personal immunity required?
Neil,
Your referenced paper concludes:
“While this cannot provide conclusive evidence that these antibody responses protect from reinfection, it is very likely that they will decrease the odds ratio of getting re-infected, and may attenuate disease in the case of breakthrough infection.”
Given the above statement does the result of the work by Wajnberg et al constitute hard evidence?
Kingsley,
“Hallelluya!”
The Aguas et al modelling estimates that 10 – 20% infection rates are required to achieve herd immunity threshold.
It also appears that C19 kills 0.5 – 1.5% of those infected.
On these figures,the least to most number of deaths required for the US (population c. 330M) to achieve HIT is between 165,000 and 990,000.
I guess you will be cracking open the champagne when US deaths have reached 990,000 because then you will know for sure that HIT has been achieved and you can safely enjoy your Christmas (that’s if you’re still around 🙂 ).
@ Neil Wilson:
“It’s very seasonal.”
July 28th: GENEVA (Reuters) – A World Health Organization official on Tuesday described the COVID-19 pandemic as “one big wave” and warned against complacency in the northern hemisphere summer since the infection does not share influenza’s tendency to follow seasons.
You better let the World Health Organisation know asap – I’m sure they’ll be happy to hear it!
Henry,
Your concerns about the duration of immunity and reinfection rates also apply to vaccines.
Hard evidence on whether immunity lasts for n years will not be available for another n years.
Meanwhile we have to make decisions based on softer, less certain, indirect evidence.
.
The other paper mentioned by Neil Wilson [Aguas et al. 10.1101/2020.07.23.20160762] has relevant analysis regarding the sensitivity of herd immunity to reinfection rates.
It notes that “Above = 1⁄* – the reinfection threshold- infection becomes stably endemic and the HIT concept no longer applies.” This is essentially your point.
However, the authors also say “Respiratory viruses are typically associated with epidemic dynamics below the reinfection threshold, characterized by seasonal epidemics intertwined with periods of undetection.”
Henry,
Reported deaths for COVID-19 are exaggerated due to the inclusion of co-morbidities, and most infections are unreported, so your assumed death rate (0.5 – 1.5% of infected people) may be too high.
.
A value judgement is that we should be more concerned with the loss of years of life rather than crude deaths.
Most COVID-19 deaths are elderly people, so the average loss of life is about 10 years per death, compared with about 40 years average life expectancy for the whole population.
Thus the percentage loss of expected life years is roughly 1/4 the death rate.
To all commentators:
I think we have had enough talking about the virus from a medical perspective, given that so little is known as yet, and this is not the place to discern the subtleties involved.
Best wishes
bill
Kingsley,
“A value judgement is that we should be more concerned with the loss of years of life rather than crude deaths.”
That is your value judgement. Not mine.
I’ve been reading this blog quite a lot during the pandemic. Most of the other things I read are now outside the mainstream media as it became clear to me, in the UK, that reporting on the pandemic was primarily an exercise in the instilling of confusion and fear, which was damaging my mental health. The insights of MMT, which appear to me to be completely convincing insofar as I’m able to follow them (lots of new concepts and vocabulary, I have no background in economics), do indeed provide a utopian perspective on how such an epidemic might be managed, but I’m not sure they lead to the conclusions Bill reaches in terms of how best to manage THIS epidemic. I come at the situation from the point of view of risk management and, if anyone’s interested, have written the blog below on what I think has happened in the UK and what could have been done differently. No doubt given (overt) widespread acceptance of MMT the entire situation would look different, and it would be legitimate to argue for an approach that saved lives, no matter the (financial) cost. But in terms of lockdown, there are other costs, which are by no means insignificant…
https://medium.com/@notthenewnormal/covid-19-a-risk-assessment-b71f3315c947
“Life” can not be measured in terms of widget A (economy) versus widget B (death rate).
Surely even an economist can get this? A person locked down is not experiencing the full richness of life. Many, would gladly sacrifice the risk of catching this virus, and others catching it, so that they can experience freedom, those who find this shocking should examine how much they really care about the lives of others, and what they ever did pre Covid to make anybodies life, other than their own, better.