It's Wednesday, and as usual I scout around various issues that I have been thinking…
Vaccine study suggests boosters will be required sooner rather than later
It is Wednesday and so just a few points today. I obviously like data as it tells me a lot about the world and often forces me to alter my views on things. While I mostly analyse economic and financial data, which is my professional skill, I also like to investigate other data sets on things that interest me. Today, I am looking into the vaccine question, which has been playing on my mind lately as the Australian political class, under pressure from all sorts of business lobby groups who fund their election campaigns, have been ‘opening up’ the economy (states and territories) despite high case numbers in some jurisdictions and despite relatively low vaccination rates. They have come up with a ‘Roadmap’ to ‘living with Covid’ (which will see many people die from Covid) and defined key thresholds in terms of average vaccination rates. The problem is the these thresholds are not very scientific at all and their semblance of ‘safety’ points is an illusion. In effect, the political class has abandoned their pretence to following health advice and are just going for it. It is a difficult period in our history.
Some Vaccine Analysis
Last week, the NSW State Government run by free marketeers ‘opened’ the economy up after weeks of lockdown due to a severe virus outbreak, which resulted from initial incompetence by the same government.
It touted that NSW had reached the celebrated ’70 per cent double dose’ threshold, that the so-called ‘National Plan’ had deemed the point when we “live with the virus”.
The next threshold is ’80 per cent double dose’ which will see almost all restrictions lifted.
The politicians have been touting these thresholds for months now as if they represent a safe passage out of the health risks of the virus.
The thresholds are a farce.
To safely achieve herd immunity against COVID-19, a substantial proportion of a population would need to be vaccinated, lowering the overall amount of virus able to spread in the whole population.
The World Health Organisation advises that (Source):
Attempts to reach ‘herd immunity’ through exposing people to a virus are scientifically problematic and unethical. Letting COVID-19 spread through populations, of any age or health status will lead to unnecessary infections, suffering and death … We are still learning about immunity to COVID-19. Most people who are infected with COVID-19 develop an immune response within the first few weeks, but we don’t know how strong or lasting that immune response is, or how it differs for different people.
They know that to achieve safe levels of immunity for polio requires 80 per cent of the population to be vaccinated, but, for measles, the figure rises to 95 per cent.
But, they admit that “The proportion of the population that must be vaccinated against COVID-19 to begin inducing herd immunity is not known.”
So it would be better to find out before adopting the “exposing people to a virus” approach becomes the norm.
Unfortunately in Australia the latter option is what the conservatives are now pushing on us. Even progressive state governments are being forced to follow the ‘live with Covid’ mantra because the spillover from the ‘freedom’ state (NSW) became difficult for other states to prevent without draconian border rules, which cannot be maintained indefinitely.
And then you think about what the 70 and 80 per cent above 16 years threshold rules actually amount to.
I did some calculations.
This graph covers the states/territories and Australia and shows the proportion of the Total populations in each jurisdiction that will be covered when the two thresholds: 70 per cent 16+ double-dosed, and, 80 per cent 16+ double-dosed, is achieved.
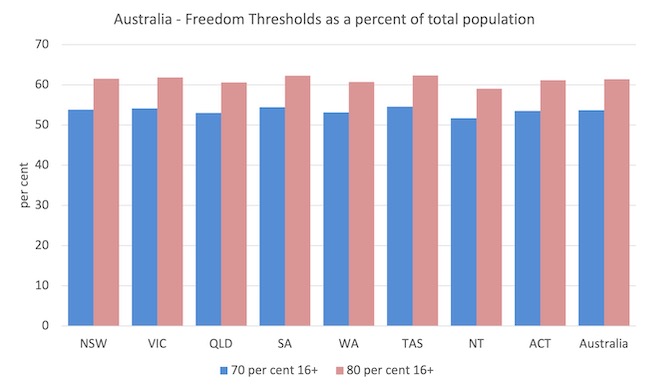
So for the nation as a whole, when the first opening up at 70 per cent double-dose for 16 years and above is achieved, the nation is only 53.7 per cent vaccinated.
And at 80 per cent 16+, the figure becomes just 61.4 per cent.
Both thresholds are below any sensible measure of ‘herd’ immunity.
At present, no-one below 12 years is being vaccinated as if the young children don’t catch and spread the virus.
I may be proven wrong and case numbers might drop significantly as the thresholds are passed.
But we have only the UK to observe and note that they are now heading back into escalating numbers and strains on the hospital system.
There has also been extreme pressure on citizens to truncate the period between the first and second innoculation injections despite the scientific evidence that this reduces the effectiveness of the vaccination markedly in some cases.
Many people are getting their second dose of AZ, the already inferior vaccine, after just 4 weeks, despite the scientists saying that maximum effectiveness comes if the doses are at least 12 weeks apart.
There are two reasons for this:
1. People have been scared by the daily press conferences and the berating from the politicians.
2. The politicians knew they could fabricate a ‘safe’ opening if they came up with these threshold vaccination targets and then hurried everybody into achieving them.
Forget the science.
Every day the politicians have been out on TV talking about the ‘Roadmap’ (to freedom) and telling us that if one had not received a double dose then they would be denied freedoms etc.
Society has been segmented into those without the double and those with.
So people who were sick of lockdown were given a massive incentive to join those with (double dose) by truncating the time period between the doses.
The politicians could then look like they were giving us back our freedoms because we were all dutifully reaching these fabricated ‘safety’ thresholds.
The problem is that now we have millions of Australians wandering around free – going to bars, parties, homes, schools etc – thinking they are fully vaccinated, when, in fact, their double dose is inferior and the antibodies will wane quickly.
The rush to do this was also pushed by the Federal government to cover up the fact that they had no ordered enough vaccine in the first place (they penny pinched on Pfizer who pushed the nation down the queue) and so the actual program of innoculation was delayed by some months as they scrambled to get more doses.
And that made the closed border issues more stark because it was simply unacceptable to ‘open up’ with low vaccination rates.
The fact that none of the journalists are pursuing this point surprises me.
I read a recent study done by the Public Health England researchers – Vaccine effectiveness and duration of protection of Comirnaty, Vaxzevria and Spikevax against mild and severe COVID-19 in the UK – which uses data compiled after 9 months of vaccine used in the UK.
Their study seeks to “estimate vaccine effectiveness over time since the second dose of Comirnaty, Vaxzevria and Spikevax in England.”
The results are interesting and highlight why we should be both careful in opening up while not falling into the short-termism of truncating the second dose interval.
1. “Vaccine effectiveness against symptomatic disease peaked in the early weeks after the second dose and then fell to 47.3 (95% CI 45 to 49.6) and 69.7 (95% CI 68.7 to 70.5) by 20+ weeks against the Delta variant for Vaxzevria and Comirnaty, respectively.”
2. “Waning of vaccine effectiveness was greater for 65+ year-olds compared to 40 to 64 year-olds.”
3. “Vaccine effectiveness fell less against hospitalisations to 77.0 (70.3 to 82.3) and 92.7 (90.3 to 94.6) beyond 20 weeks post-vaccination and 78.7 (95% CI 52.7 to 90.4) and 90.4 (95% CI 85.1 to 93.8) against death for Vaxzevria and Comirnaty, respectively.”
Here are some graphs I produced from the data provided in the Study.
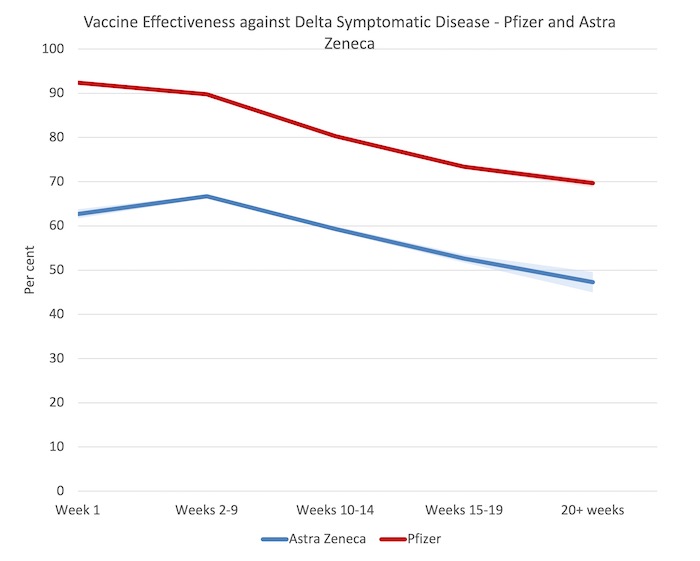
The first one shows the effectiveness against Delta symptomatic disease from Weeks 2-9 after the second dose to 20+ weeks for Astra and Pfizer. The shaded areas are the 95 per cent confidence intervals, whereas the lines indicate the mean estimate from the regression models.
So the CIs indicate that we can be 95 per cent sure that the true result lies within the range. It also means, for example, that we are indifferent between that level of confidence between, say, Astra Zeneca being 52.7 per cent effective against Delta death after 20+ weeks and 78.7 per cent effective.
The points to observe are:
1. A fairly rapid waning in effectiveness in both vaccines.
2. After 20+ weeks, a person who has followed the Astra Zeneca routine is less than 50 per cent protected against symptomatic illness from Covid. For Pfizer, the drop is to 69.7 per cent effective.
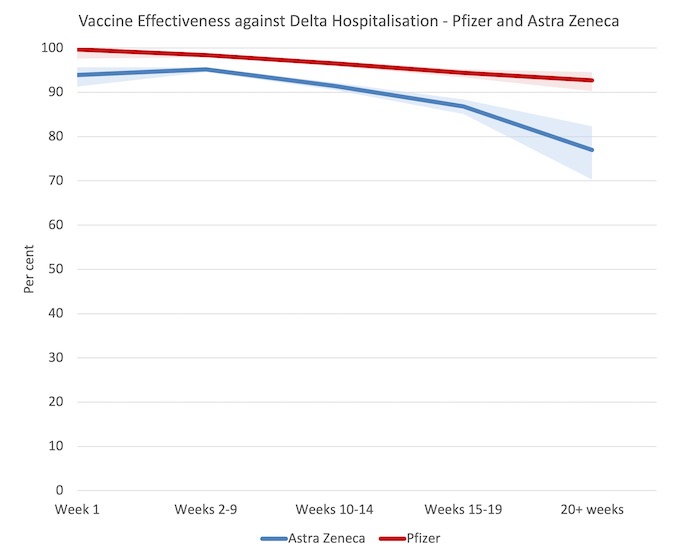
The next graph shows the effectiveness against Delta hospitalisations from Weeks 2-9 after the second dose to 20+ weeks for Astra and Pfizer.
The points to observe are:
1. Even though the effectiveness against disease wanes substantially, the chances of ending up in hospital decline less.
2. Both vaccines are very effective in this regard.
3. The authors write:
Our study provides evidence of significant waning against symptomatic disease but limited waning against severe disease over a period of at least 5 after administration of second doses in a programme with an extended interval between first and second doses. Waning appeared to be greater in older age groups and among individuals in clinical risk groups, suggesting that these individuals should be prioritised for booster doses.
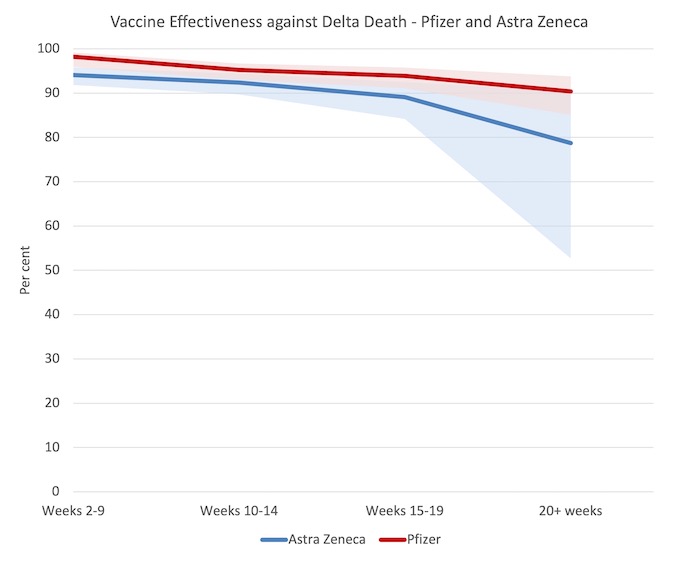
The final graph one shows the effectiveness against Delta deaths from Weeks 2-9 after the second dose to 20+ weeks for Astra and Pfizer.
The points to observe are:
1. Anyone who has taken AZ has an almost 50-50 chance of dying after 20+ weeks of receiving the second dose if they get sick. That is not a very ‘safe’ position to be in.
The study also found that truncating the period between doses significantly reduced the effectiveness of the vaccines, other things equal.
For example, for Pfizer, the effectiveness from symptomatic disease dropped from over 60 per cent to less than 40 per cent in people aged 80+ after 25+ weeks after second dose (the intervals were large and overlapping though).
The main message from the study, is that we cannot conclude that we are safe after two doses of either vaccine and booster shots will be necessary to increase the longer-term effectiveness as the 2-dose effectiveness wanes after 20+ weeks.
Of course, with the first world looking after themselves and allowing the companies to maintain patents, the idea that the advanced nations should be boosting while the poorer nations are enduring such low levels of first round vaccinations is somewhat difficult to cope with.
The reality is that billions of doses are necessary to be distributed everywhere as a matter of priority.
Music – Wes Montgomery and Clark Terry
This is what I have been listening to while working this morning.
This is from the 1992 album – Straight, No Chaser – which was recorded on the Dutch Radio VARA on April 2, 1965 at their Hilversum studios.
One of my closest friends, now deceased, worked at the studio on these sorts of projects for many years. I miss him.
The album was released in 1988 as “VARA Radio – 1965” on Vara’s own jazz label.
The interesting thing is that Wes Montgomery only visited Europe once over the course of his career (which was short anyway).
His Paris concert in March 1965 was a classic and features Wes and flugelhorn player Clark Terry.
This track – Just Friends – was the peak of their partnership.
The players are:
1. Wes Montgomery – guitar.
2. Clark Terry – flugelhorn.
3. Ruud Jacobs – double bass.
4. Han Bennink – drums.
5. Pim Jacobs – piano.
Anyway, this is one of the best versions of this jazz standard.
I loved the way Wes Montgomery played without a pick and achieved that really sombre yet clean sound on his octaves. I have never really been able to replicate that level of clarity in that context but it doesn’t stop me trying to mimic his genius.
That is enough for today!
(c) Copyright 2021 William Mitchell. All Rights Reserved.
The first generation of vaccines are not sterilising and were never designed to be. So they are unable to stop the spread of the disease, only the severity of its impact on the individual.
Given the technology we have, in areas where Covid is now endemic, if we were rational we would want to catch Covid about three weeks after the (correctly administered) 2nd dose. That would induce full sterilising immunity.
And you’d want to do that because this is a disease where the risk increases as you get older. Which means you want to catch it today, not tomorrow.
Can’t see Covid parties catching on though.
The first thing to point out is that the shots we currently have (all of them) are not vaccines, in the sense that they do not vaccinate people against the disease Covid19. After taking these shots, you can still catch Covid and spread it to others.
Just as we do not have a vaccine for the common cold or for AIDS, we do not have (as yet) a vaccine for Covid19. What we have has been described as ‘experimental gene therapy’. the full effect of which on the human population is not yet known.
The second thing to notice is the incredibly concentrated messaging effort of a combined Big Govt, MSM, Big Tech, Big Med and Big Pharma. Its almost enough to make one suspicious.
Overall, this is an excellent post by Bill. First, I just want to question one point where there may be an error. The final graph has this statement above it:
“1. Anyone who has taken AZ has an almost 50-50 chance of dying after 20+ weeks of receiving the second dose if they get sick. That is not a very ‘safe’ position to be in.”
This doesn’t seem correct to me, unless it is effectiveness against Delta death AFTER requiring hospitalization. The graph does not even support this interpretation if one follows the solid line for AZ. Only taking the lower bound CI shading would support this contention.
Please correct me if I have misinterpreted the statement and graph. Overall, as I say, I consider this an excellent post. But rather than write more about it at this stage, I just want to see if I am on track or off track on the issue of the last graph. Should the last graph be titled something like “Vaccine Effectiveness Against Delta Death For Serious Cases Requiring Hospitalization”? Is that what the last graph shows? Also, have I misunderstood the CI shading if that is what it is or is not?
“Anyone who has taken AZ has an almost 50-50 chance of dying after 20+ weeks of receiving the second dose if they get sick. That is not a very ‘safe’ position to be in.”
Hmmmm. I think this is mistaken.
The infection mortality rate, without vaccination, is only a few percent. It certainly doesn’t increase if you’ve been vaccinated.
I think what is meant is that 100% protection against dear, post vaccination, means you don’t die. 0% protection means you are no better off than not having been vaccinated. So 50% would mean that the infection mortality rate would be halved, perhaps to around 1% (highly dependent on age). Whilst a 1% death rate is worrying it is not nearly 50%.
“The first thing to point out is that the shots we currently have (all of them) are not vaccines”
Vaccination has become an Humpty Dumpty term – like full employment
Hence why the CDC changed the definitions to
https://www.cdc.gov/vaccines/vac-gen/imz-basics.htm
from
https://web.archive.org/web/20191111050113/https://www.cdc.gov/vaccines/vac-gen/imz-basics.htm
Have you checked out the stats for adverse reactions?
Tim Borer has hit the nail on the head. And Bill has been consistently technically correct in always referring to “effectiveness” right through his post. However, I do think this specific sentence of Bill’s does need re-phrasing as it seems to give the wrong inference:
“Anyone who has taken AZ has an almost 50-50 chance of dying after 20+ weeks of receiving the second dose if they get sick.”
People like me need to go back to Vaccinology 101, especially as I never did such a course. (I did do cellular biology (Cell Biol) 101 many years ago.) It’s time for some definitions. I got them from the Canadian Center for Vaccinology, Dalhousie U., Halifax.
“Vaccine efficacy – % reduction in disease incidence in a vaccinated group compared to
an unvaccinated group under optimal conditions.
“Vaccine effectiveness – ability of vaccine to prevent outcomes of interest in the “real world””
The scare quotes on “real world” make sense as there are many real world milieus in the enviromental, built environment, social and economic senses. The second definition elides the statement “% reduction in disease incidence”. This is unfortunate but it is clear that the same concept is intended. Thus, Tim Borer is correct to say:
“50% (effectiveness) would mean that the infection mortality rate would be halved”.
None of the above affects the overall tenor and conclusions of Bill’s original post. Bill is correct at every point to be greatly concerned. These vaccines are fairly effective but far from perfect. And the waning of protection by 20 weeks for Delta variant is very concerning. The number of cases, including morbidity and deaths, that we will see from an outbreak where only about 66% (at best!) of the total population is protected (and then not perfectly) will likely be quite high. One third of the population unprotected is still over 8 million people. Assume 4 million of these have significant vulnerability by reason of age or pre-existing conditions. Assume just 1% of these people die. That would be 40,000 people. Then we can add in some from the vaccinated group and some more from new imported strains which will come in for sure. Add another 10,000 estimated. We could be looking at 50,000 deaths in the next two years.
There are some suggestions now that long covid from Delta is affecting up to 50% of the non-vaccinated. I haven’t seen data on long covid for the vaccinated. Long covid can last weeks to months and can occur from mild as well as severe infections. This is uncharted territory.
Bill also notes: “The second thing to notice is the incredibly concentrated messaging effort of a combined Big Govt, MSM, Big Tech, Big Med and Big Pharma. Its almost enough to make one suspicious.” I agree and will offer some thoughts at some point.
I will also note here that the next 6 months to 2 years may well be the most dangerous time for Australians, including vaccinated Australians! We will actually become less safe if everyone, people and government, start acting like vaccination is an impenetrable shield. COVID-19 vaccination to date is far from that. The vaccines are decidedly leaky. Older Australians and anyone with a pre-existing medical condition will have to re-double ALL their personal measures, meaning masking, hand cleaning, avoiding crowded venues and maybe even maintaining a degree of self-imposed isolation especially if one is older (than say 60) and/or immune-compromised. This is going to be a very dangerous time. I implore everyone to maintain vigilance and self care.
Looks like Australia is directly following the UK’s libertarian playbook. What an appalling example to give to the world – and how furious I am to be one of Johnson’s/Javid’s guinea pigs.
Morocco has just banned British visitors. The rest of the world would be doing us a massive favour if it followed suit. Perhaps then the UK govt might be pressured to change its tune if its citizens – sorry, subjects – cannot ever travel beyond our borders??
A Senate committee in Brazil has announced that it will attempt to charge Bolsonaro with murder, following the deaths of 600,000 citizens. What a great precedent to set; if there’s any justice in the world then Johnson, Sunak, Hancock and Javid will be joining him in the dock.
Tim Storer and Ikonoclast got there before me, but yes, the ~50% declining protection of vaccines is a percentage to be applied to the *existing risk of death* ( around 2%… so reduced to 1%), and not to infection – which would indeed be terrifying!
I had Covid-19 in January 2020 and recovered without hospitalisation aged 67, in the UK. Subsequently, I joined a UK COVID research programme which finally was able to blood test me in January 2021. They confirmed my antibody status was high, and that I had indeed had Covid. My UK GP insisted I still needed to be vaccinated, though I didn’t see any point as I know enough about vaccinology (in dogs ) to know my immune system would shrug off the vaccines as it would recognise the virus. Two AstraZeneca jabs 9 weeks apart later, the research people blood tested me again in June 2021. Result? My antibody levels are still high. In other words, for me nothing has changed.
Like Bill, I smell a money rat operating an international racket more designed to enforce compliance than protect people. What about all the people who can’t be vaccinated? There is no such thing as 100% vaccinatable people. Sick people cannot be vaccinated, vaccines are only licensed for use in healthy people (the same applies to dogs). The reports of adverse vaccine events are running into the thousands, with more than 1,000 deaths reported following vaccination. Some have reported losing their hearing, or their sight.
Here in Blighty, we are currently on a reported 49,000 new covid cases per day (an extremely dodgy, probably large underreporting) and 179 new daily deaths, moving in an upward direction. There isn’t any reporting that I know of numbers given a booster jab to protect them better through the winter, against numbers becoming less protected as their original doses become less effective. Last winter we had hardly any flu cases and hospitalisations because we did have a certain amount of mingling reticence and mask wearing. Flu jabs for the over 50s seem to be slow. Catch covid + flu significantly increases serious illness.
@ Valerie Leppard re: ‘The reports of adverse vaccine events are running into the thousands, with more than 1,000 deaths reported….’ I’m skeptical of govt figures, but I’m even more skeptical of other figures ‘reported’.
I agree absolutely that data gives us answers, and I applaud the data driven analysis here but I am going to disagree with the assumptions and the conclusions of the modelling.
The term herd immunity” is about as useful to covid as the analogy of household budgeting is to fiat currency issuing governments. It doesnt exist for Covid and you can really only employ it for a very few infectious agents- say for measles which has an unchanging haemagluttin protein that means infection and immunization gives almost life long immunity. 9 months after contracting Covid you are almost as likely to catch it again as someone who has never been infected. Everyone in the world will meet Covid if not this year then the next or the one after that. Having it once is no better than having had the flu in terms of protection. Getting vaccinated one year doesnt mean you dont need to get vaccinated the next. Its a never ending battle between evolution and human ingenuity. This is not in any way to underestimate the wonderful benefits of vaccination and the lockdowns and so on which have bought us an incredibly useful 18 months of Covid zero. Also now there are at least 6 effective treatments for those infected meaning prognosis has improved by about 50% irrespective of vaccination.
the models are just that – models with all their limitations. I am sure even the people who put them out dont have any confidence in their accuracy. Just have a look at all the predictions over the last 2 years. They are only good for 6 weeks at the most. Probably worse than economic models which have better data and in which virus evolution is not an issue. The virus now is different to that upon which the models are based on and will be different again next year. Human response to the pandemic has altered along with government edict. The vaccines will be different next year. Anyone who tells you they know what is going to happen with Covid in 6 months is having themselves on – yet we live in world that in contrast to the past, expects experts to provide accurate predictions of future events.
“The first thing to point out is that the shots we currently have (all of them) are not vaccines”
So, apparently, the flu vaccine is not a vaccine? Seeing as the flu vaccine predates any vaccines that eradicated any viruses (e.g. polio, smallpox), I think it’s safe to say that any definition that a vaccine has to provide full asymptomatic immunity with no exceptions is fallacious.
Covid isn’t likely going away anytime soon. The vaccines at least are capable of greatly reducing morbidity and mortality, that much is very evident in the statistics from areas were the vaccination rate is high, and it appears that while antibodies do wane over a few months the immune system does retain the memory of covid and hence the capacity to produce new antibodies fast enough to prevent severe illness for quite some time, possibly permanently.
We will however probably have to accept that we will get flu like illness more often as the price of getting back to normal.
“The fact that none of the journalists are pursuing this point surprises me.”
Australian journalists are just as corrupt and in the pocket of government as they are in the UK I take it. It appears the mission of everyone involved in corporate media is to no longer pursue the truth, but to act as propagandists for their mates in the Establishment.
Why do we have to vaccinate against flu every year although it is by large the same H1N1 of the Spanish flu from 1918? Because the fast mutation rate of viruses shortens the best before date of the vaccines. Vaccines on their own cannot beat viruses. It applies equally to the natural heard immunity.
We cannot catch and kill viruses like gnats that carry malaria or rats and flees that carry plague. All reasonable action against viruses is based on probability and statistics. One virus does not make ill, but the required amount of viruses that creates sickness is different for everybody. To fight viruses we have to keep the amount of viruses that enter our bodies as low as possible and stop new variants from spreading all over the world. Whatever Pfizer is, produced by conventional methods or some other ways, it reduces the probability of falling ill. But people also need to wear masks, wash hands and shopping, keep social distancing and stop travelling.
This pandemic is different from the previous ones because all the big towns, the petri dishes of Corona mutations, are interconnected with busy airlines. These are mostly civil servants and business people who want to travel and do not want to sit the full time in quarantine. Even when one country rids itself from virus, like Vietnam and New Zealand almost managed to do, they cannot protect themselves from new variants, stronger and more aggressive, if they continue receiving people from abroad without strict quarantine regime.
Estonia uses mostly Pfizer and Astra Zeneca. About half of population is fully vaccinated. Almost constant one third of all the infected people are fully vaccinated. These numbers are reported every day on the home page of our Health Board. The percentage of the unvaccinated people among the dead is even less, I would estimate it about 5%.
I do not understand the puzzlement over the Japanese success in beating Covid19. Whoever watched the ceremony of passing the Olympic flag from Tokyo to Paris saw that all Japanese, from children to adults, were wearing masks. Very few in the French crowd did. In Japan already little children wear masks. In Estonia younger children do not wear masks even when their parents and older siblings do. A toddler in mask is a rare sight here.
What is the probability to be hit by lightening in an empty field in thunderstorm? What is the probability of getting virus infection? The problem is that virus does not warn people with spectacular visual and acoustic effects.
In precarity governance, what we are practicing now, crises are not to be beaten nor reversed, but sustained instead. Crises keep people in line, keep them busy.
This whole arena is fraught with misinformation and false beliefs. We need to be careful to stick to known facts. At the same time, we need to remember that facts, in complex arenas, are not simple and often can only be expressed in probability terms. We don’t have certain knowledge, we have only likely or probable knowledge to degrees of certainty. In stating the items below, I am not saying that people writing above denied them but many people out in the community have denied them.
1. The SARS-CoV-2 virus which causes COVID_19 disease is real. It has been gene sequenced. It also mutates relatively rapidly for a coronavirus and many mutations have been gene sequenced.
2. The issue of what a vaccine is, is definitional, but most vaccines have never given absolute 100% immunity. But high vaccination rates (usually 90% plus) plus high vaccine immunity rates (usually 90% plus) can break the infection cycle in a population and eradicate a disease. However, with a highly transmissible disease with an aerosol-pulmonary infection route, eradication becomes even more difficult. SARS-CoV-2 virus, Delta variant, is now the second most infectious pathogen known to science, after emerging less than two years ago and continuing to evolve.
3. The mRNA vaccines against SARS-CoV-2 are quite effective as per the percentages and probabilities shown in the graphs Bill created from the data of one of the latest UK studies (not yet peer reviewed but likely reliable). The vaccines are not perfect and immunity wanes significantly by the 20 week mark. All shown well by Bill’s graphs.
4. These vaccines have risks and the official figures do appear to understate the risks, more so in their summaries than in the deep data if you dive into it. But even the deep data appears to be affected by the setting of the “proof bar” for vaccine caused deaths and other side-effects at a high level. How much this effect operates is hard to tell. How comprehensive the data is, is also hard to tell.
5. The SARS-CoV-2 mRNA fragment in the Pfizer vaccine (for example) is extraordinarily unlikely to change human DNA in the vast majority of the vaccinated. The vaccine only uses a fragment of the SARS-CoV-2 RNA anyway and this fragment encodes for the viral spike protein only. In addition, the viral spike protein that the vaccine’s altered RNA encodes for is NOT the precise spike of the live virus. The vaccine-encoded spike protein has a 2-P (proline) addition to render it inactive at attaching to human cells. But it does still activate immune responses in the blood stream and that is the design intention of course. The RNA fragment in the vaccine slips into muscle cells at the injection site simply because it is so small. It needs no spike proteins for entry as does a virus capsule with a full RNA strand inside.
I’m going to hope that bill @2:27 is not Bill Mitchell.
So 3000+ people have had the worst kind of adverse reaction to a covid-19 vaccine and died. I can believe that. Since about 3.77 billion people have received at least one shot. Makes your chance of croaking from the vaccination less than 1 in a million. Covid-19 has killed more than 1 out of every 500 people in the United States. One in a million, or one in 500- compare those odds. I would get the shot. Oh- I did- and seem to be doing just fine six months on.
I tend to defer to the opinion of a close relative on these matters – given that he has been a practicing medical doctor for more than 40 years. If the vaccines were not generally safe and effective he would never recommend that his own relatives receive them.
I tend to regard claims that there are massive numbers of casualties of dangerous vaccine side-effects being hidden with some scepticism (while acknowledging that side-effects can and do occur) for the same reason I dismiss claims that the virus does not exist or is no worse than the common cold – such a deception would require the co-operation (either willing or coerced) of literally millions of medical professionals.
Around 2 billion doses of the vaccines have now been administered – how does one go about hiding large numbers of serious injuries and deaths caused by vaccine side-effects from millions of doctors whose job it is to administer the vaccines and to treat those presenting with side-effects or any illness at all? If there are, why aren’t doctors speaking out en masse? Have they been cowed into silence? Are they evil conspirators themselves?
I’m going to require rather more evidence before I’ll consider that my own relatives in the medical profession are either wrong about the vaccines or are not the people I have always thought they were.
@Ikonoclast ‘in silico’.